
UN Women has been closely following the political and economic response to COVID-19 and how it is impacting women and girls. We are working with partners to deliver a more accurate picture of the gender dimension to the response so that it can be more effective for women and girls.
Collaboration with WHO
UN Women and WHO join forces to bridge the gender data gap and provide latest available data on COVID-19 cases by sex and age. As more gender data is produced and disaggregated, we will make it available here.
Update on Rapid Assessments
Surveys show that COVID-19 has gendered effects in Asia and the Pacific
Guidance: Rapid gender assessment surveys on the impacts of COVID-19
Related stories
COVID-19 and gender: What do we know; what do we need to know?
COVID-19 sends the care economy deeper into crisis mode
COVID-19 may be prompting men to help out at home, evidence from the Maldives suggests
COVID-19 continues to spread
The COVID-19 virus continues to spread rapidly around the world. In just a few months more than 200 countries and territories have reported cases, resulting in xx million people infected globally. The death toll currently stands at xx. Here is what the situation looks like today.
Live tracker: COVID-19 cases around the world
Source: WHO, CDC, ECDC, NHC, DXY, 1point3acres, Worldometers.info, BNO, state and national government health departments, and local media reports, as compiled by Johns Hopkins CSSE.
Notes: The designations employed and the presentation of material on this map do not imply the expression of any opinion whatsoever on the part of UN Women concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. For full list of notes on data and data sources see Johns Hopkins CSSE. The map is maintained in near real time throughout the day through a combination of manual and automated updating. The time of the latest update is noted on the bottom of the dashboard. The GitHub database updates daily at around 11:59 p.m. UTC. Occasional maintenance can result in slower updates.
Emerging data by sex and age
The virus does not discriminate. In order to respond effectively to the crisis, we need a whole-society approach to understand its differential impact on women and men. Supporting gender analysis and sex-disaggregated data is an integral part of a strong COVID-19 response.
COVID-19: Sex-disaggregated case data (provisional analysis)
Source: Data submitted to NCOVmart reported through the global surveillance system of WHO, as of 10 am 18 January 2021.
Notes: Data cleaning are ongoing and in progress. All numbers should be interpreted with caution. As of 10 am 18 January 2021, 93,194,922 cases were reported. Data presented here, therefore, represent only 19% of all reported cases. The data by sex and age shown here are based on reporting from 137 countries, areas and territories.
COVID-19 cases, by age and sex (provisional analysis)
Source: Data submitted to NCOVmart reported through the global surveillance system of WHO, as of 10 am 18 January 2021.
Notes: Data cleaning are ongoing and in progress. All numbers should be interpreted with caution. As of 10 am 18 January 2021, 93,194,922 cases were reported. Data presented here, therefore, represent only 19% of all reported cases. The data by sex and age shown here are based on reporting from 137 countries, areas and territories.
In focus: Health-care workers
In some countries, COVID-19 infections among female health workers are twice that of their male counterparts. Governments should ensure that all care-sector professionals, and health-care and long-term care workers in particular, have adequate protection against transmission.
Infections of health-care workers: The case of Spain
Source: UN Women calculations based on data from Spain’s Ministry of Health, "Análisis Epidemiológico COVID-19". Latest data available as of 30 April 2020.
Infections of health-care workers: The case of Italy
Source: UN Women calculations based on data from Italy’s Instituto Superiore di Sanita, "Report bisettimanale". Latest data available at 4.00 PM on 28 April 2020. The number of infected health workers by sex has been derived using the total number of infected health workers and the percentage of infected male health workers.
Infections of health-care workers: The case of United States
Source: CDC. 2020. “Characteristics of Health Care Personnel with COVID-19 - United States, February 12-April 9, 2020“. Accessed 4 May 2020.
Sex-disaggregated case data for select countries
Source: Global Health 50/50. xx
Note: Data are collected from official government sources and compiled by Global Health 50/50. The total number of cases and deaths reported here may not reflect the current number of cases and deaths, as they are reported from the date that sex-disaggregated data was last available. They may also only reflect a subset of data where countries have reported sex-disaggregated data. Definitions of cases and deaths recorded due to COVID-19 may vary by country.
Health systems are strained
The surge in COVID-19 cases is straining even the most advanced and best-resourced health systems to the breaking point. As the virus spreads there are real concerns about the ability of developing regions, with already weak health-care systems, to cope. We know from past disease outbreaks that access to prenatal and maternal care services and frontline response to gender-based violence suffers in these situations as resources are diverted elsewhere.
Health-care resources, by country and geographic region
Source: WHO 2020. Electronic State Parties Self-Assessment Annual Reporting Tool (e-SPAR). Accessed 1 March 2020 https://extranet.who.int/e-spar; World Bank 2020. World Development Indicators. Accessed 1 March 2020. https://databank.worldbank.org/source/world-development-indicators; UNSD 2020. Global SDG Indicators Database. https://unstats.un.org/sdgs/indicators/database.
Notes: Global and regional averages shown in red and brackets should be treated with caution as the data coverage is below UN Women's threshold (at least 50 percent of countries and/or 66 percent of the population covered). Last Updated: 04 April 2020
The takeaway
Governments are responding under huge pressure to act fast, and this sometimes means that they may act without considering diverse perspectives, including gender. For instance, stay-at-home orders limit the spread of the virus, but can potentially result in dangerous situation for women with violent partners.
Decisions that are informed by accurate data and include a gender perspective are more likely to be effective. That is why we are cooperating with decision-makers to ensure gender is integrated in national and sub-national COVID-19 response plans, not only to achieve better outcomes for women and girls, but to achieve better outcomes for everyone.
Using data to drive gendered responses to the COVID-19 crisis
10 key policy priorities
29 indicators for a data-driven response
UN Women has been closely following the political and economic response to COVID-19 and how it is impacting women and girls. It is our job to support governments to uphold the rights of women and girls – something that is even more urgent in times of crisis. Governments are responding under huge pressure to act fast – which in many cases has meant acting without considering important perspectives, including gender. Gender-blind decisions and policies are not only worse, they usually fail. What’s more, decisions that are not informed by accurate data are more likely to be ineffective. That is why we are cooperating with decision-makers to ensure that gender is integrated in national and subnational COVID-19 response plans, not only to achieve better outcomes for women and girls, but to achieve better outcomes for everyone.
To this end, there are 10 key points we are asking those who lead governments, municipalities, parliaments and other decision-makers to consider. For each policy priority area we provide an array of relevant data, statistical indicators and other data that can be used to support country-level assessment and response. This page will be updated frequently as more data and research becomes available, particularly on the gendered impacts of the pandemic and the efforts to address them.
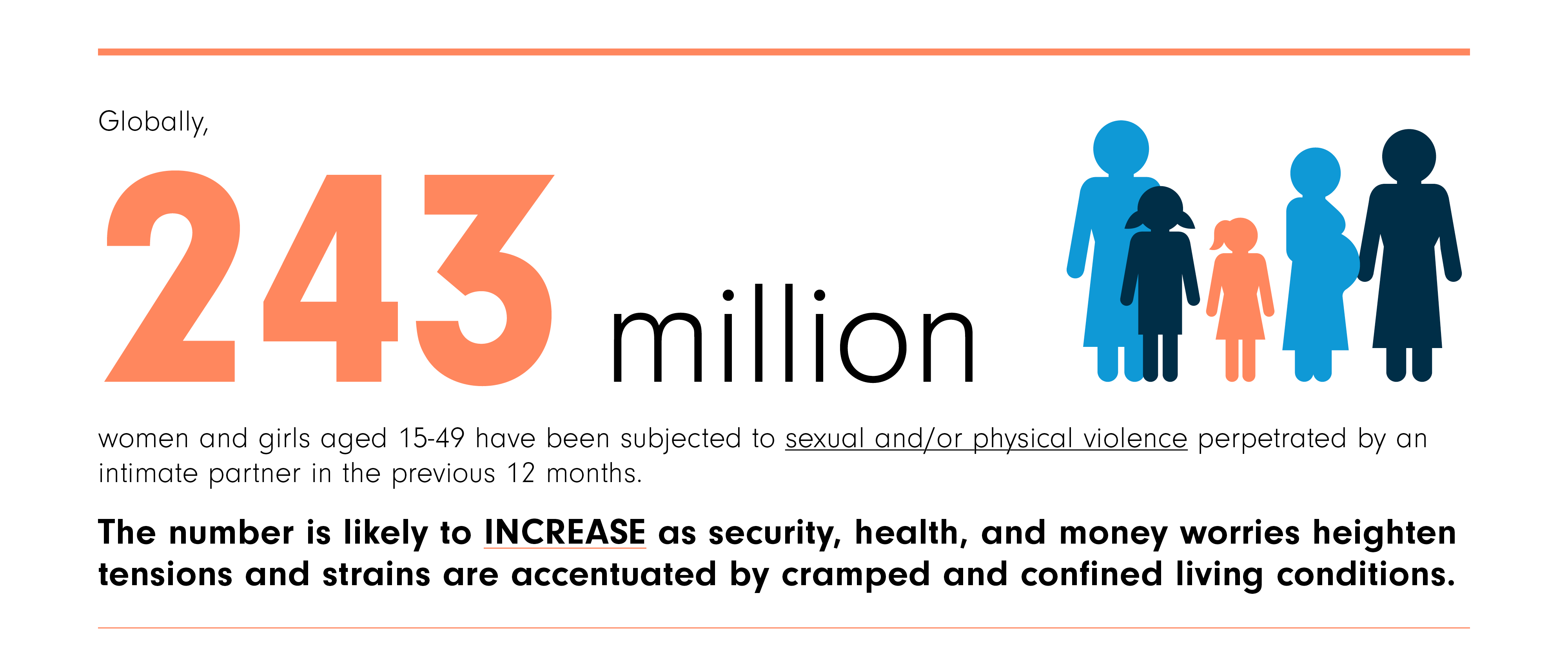
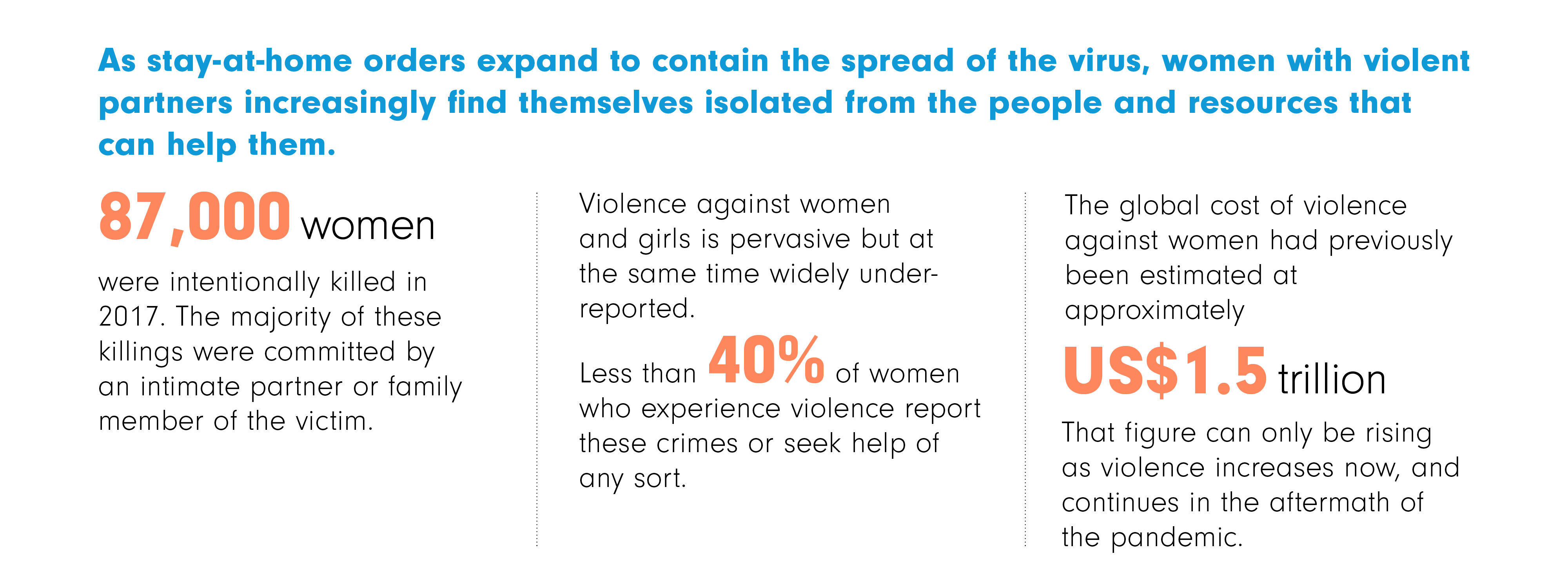
1. Home is not always the safest place for women.
As stay-at-home orders expand to contain the spread of the virus, women with violent partners increasingly find themselves isolated from the people and resources that can help them. Globally, 18% of ever-partnered women and girls aged 15–49 have experienced physical and/or sexual violence at the hands of a current or previous partner in the previous 12 months.
Policy priorities
Governments must include essential services to address violence in COVID-19 response plans, ensuring that violence survivors have access to hotlines, shelters and other protection services in the context of social distancing. Police should also continue to prioritize reports of domestic violence.
Indicators
1. Proportion of ever-partnered women and girls subjected to physical or sexual violence by a current or former intimate partner in the previous 12 months
2. Total number of female victims of intentional homicide per 100,000 population (SDG 16.1.1)
2. Women in the informal economy are especially vulnerable.
With economic activity coming to a halt, the informal sector will be the hardest hit. There are huge inequalities between women and men in terms of access to decent work and associated benefits – such as access to health insurance, unemployment benefits and other social protection. Out of the two billion workers in informal employment worldwide, just over 740 million are women.
Policy priorities
Governments should provide income support for women working in the informal sector or with vulnerable formal-sector jobs.
Indicators
3. Proportion of informal employment in non-agriculture employment, by sex (ILO harmonized estimates) (%);
4. Share of own-account and contributing family workers in total employment by sex (%)
3. Women in poverty or without an independent source of income face greater risks.
Poverty heightens the exposure and impact of COVID-19 as poor people are unable to stock-up on essentials and can’t afford to stay home. More women live in poverty than men: 50 million women aged 25–34 compared to 40 million men of the same age. Prime working-age women, especially those in a relationship and with children, are also less likely to have a job than men.
Policy priorities
To mitigate women’s economic dependence on men, governments should target individuals rather than households when implementing direct cash transfers. Policies should also address vulnerabilities of the extreme poor living in settings with inadequate water, sanitation and hygiene facilities.
Indicators
5. Labour force participation rates of persons aged 25–54, by household type (lone person household, couple only, couple with children under 6) and sex (percentage)
6. Percentage of women employed in the 12 months before the survey who worked for cash
7. Proportion of urban population living in slums, informal settlements or inadequate housing
8. Urban slums sex ratio for individuals aged 15-49
9. People with basic handwashing facilities, including soap and water (% of population)
10. Proportion of the population living below the international poverty line by sex and age (0-14 years and 15+) (Global and regional figures only)
4. Lone-mother families are more likely to be poor.
The reasons for this include fewer income-earners in the household and women’s lower wages, compared to men.
Policy priorities
Governments should consider interventions to guarantee income security and address other challenges faced by single parents, the majority of whom are women.
Indicator
11. Lone-mother households as a share of total households (%);
12. Lone-mother households, (in millions)
5. Elderly women and men are at a higher health risk from COVID-19.
Women represent the majority of the elderly around the world, especially those over the age of 80. They tend to have lower pensions, if any, and fewer possibilities to access care and other services.
Policy priorities
Governments should prioritize the care needs of older persons living alone or in residential care, particularly those without access to services and resources.
Indicator
13. Share of population above statutory pensionable age receiving an old age pension by sex (%)
14. Share of one-person households headed by females aged 60+ as a proportion of all households
15. Number of one-person households headed by females aged 60+
6. The majority of front-line health workers – especially nurses – are women, increasing their risk of infection.
Women represent 70% of workers in the health and social sectors. Women also perform the bulk of unpaid care and domestic work in homes, including caring for sick family members.
Policy priorities
Governments should ensure that all care-sector professionals – health-care and long-term care workers in particular – have adequate protection against transmission.
Indicator
16. Share of women employed in human health activities (%)
7. In many countries, fewer women than men have health insurance and access to care.
Women and girls have unique health needs, but they are less likely to have access to quality health services, essential medicines and vaccines, maternal and reproductive health care, or coverage for routine or catastrophic health costs, especially in rural and marginalized communities.
Policy priorities
Governments should ensure that all citizens can be tested for COVID-19 and access quality health-care services. This is particularly urgent for pregnant women, who still risk dying during childbirth.
Indicator
17. Universal coverage of essential health services index (0-100)
18. Access to laboratory testing capacity for priority diseases (20-100)
19. Proportion of women making their own health decisions, aged 15-49 (%)
8. Women are overrepresented in low-paid work and the pay gap remains pervasive.
Women are more likely to work part-time, in non-standard employment and on average earn less than men (for work of equal value).
Policy priorities
Governments should support vulnerable workers, especially women in low-paid, low-quality and sometimes hazardous jobs, and significantly improve their working conditions and salaries.
Indicator
20. Gender wage gaps (hourly wages SDG 8.5.1) (%)
9. Countries around the world are closing schools.
According to recent estimates, more than a billion students are out of school due to COVID-19. Those with the resources may be moving to online or remote teaching. Before the crisis, an estimated 32 million girls of primary school age were out of school compared to 27 million boys. Girls from poor and rural areas face an especially uphill battle.
Policy priorities
Governments should ensure that girls are not finding themselves caring for younger siblings or other relatives while boys continue to study. Boys and girls expected to continue schooling online should have equal access to computers and education resources.
Indicator
21. Global monitoring of school closures caused by COVID-19 – Estimation of affected learners, by sex.
10. The surge in COVID-19 cases is straining even the most advanced and best-resourced health systems to the breaking point.
We know from past experience, including the Ebola outbreaks, that access to prenatal and maternal care suffers in these situations as priorities are diverted elsewhere.
Policy priorities
Governments must ensure that despite the strain on health systems, maternal care services continue to operate safely for staff and mothers and that policies are in place to protect women’s health, including the health of pregnant women and their newborns.
Indicator
22. Planning for emergency preparedness and response mechanism (0-100)
23. Management of health emergency response operation (0-100)
24. Emergency resource mobilization (0-100)
25. Proportion of births attended by skilled health personnel (%)
26. Maternal mortality ratio (per 100,000 live births)
27. Hospital beds (per 1,000 people)
28. Physicians (per 1,000 people)
29. Nurses and midwives (per 1,000 people)
Violence against women and girls data collection during COVID-19
This brief paper summarizes principles and recommendations to those planning to embark on data collection on the impact of COVID-19 on violence against women and girls. It was informed by the needs and challenges identified by colleagues in regional and country offices and has benefited from their input. It responds to the difficulties to adhere to methodological, ethical and safety principles in the context of the physical distancing and staying at home measures imposed in many countries.
This document was developed under the UN Women-WHO Global Joint Programme "Strengthening methodologies and measurement and building national capacities for violence against women data".
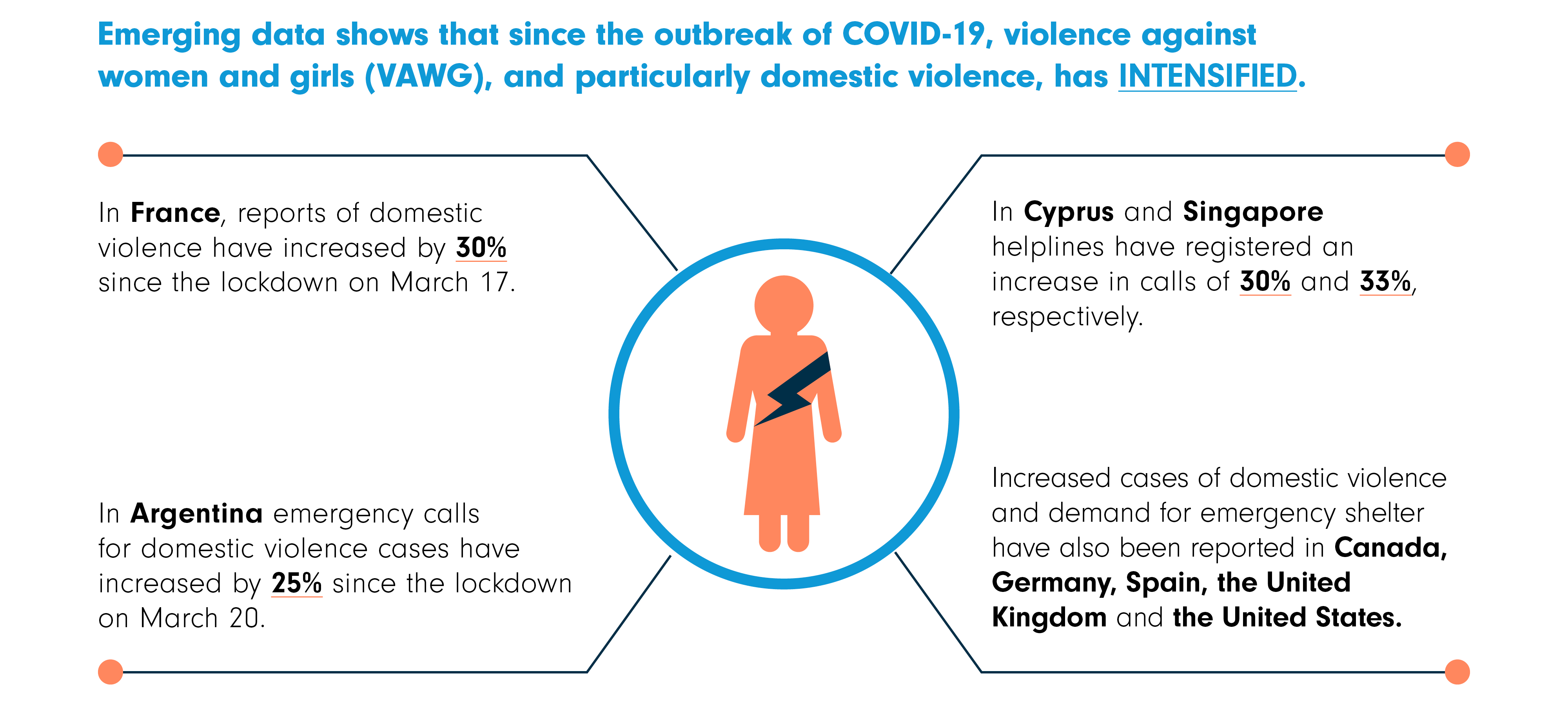
The shadow pandemic: Violence against women and girls and COVID-19
UN Women has produced a brief highlighting emerging evidence of the impact of the recent global pandemic of COVID-19 on violence against women and girls. The brief makes recommendations to be considered by all sectors of society, from governments to international organizations and to civil society organizations in order to prevent and respond to violence against women and girls, at the onset, during, and after the public health crisis with examples of actions already taken. It also considers the economic impact of the pandemic and its implications for violence against women and girls in the long-term. The infographic below provides a snapshot of the issues covered in the brief.
Download the brief
Download the infographic
Note: This brief is a living document that draws upon the knowledge and experience of a wide range of experts who support solutions to end violence against women and girls, attentive to the country context in which the crisis is occurring.
UN Women and its partners have compiled a comprehensive list of resources covering a variety of issues related to the gendered impacts of the COVID-19 crisis. The list will be regularly updated as more information becomes available.
Gender equality and the COVID-19 pandemic
COVID-19: the gendered impacts of the outbreak (The Lancet)
The gendered impacts of the outbreak (WHO)
COVID-19: A gender lens: Protecting sexual and reproductive health and rights, and promoting gender equality (UNFPA)
The Coronavirus Is a disaster for feminism (The Atlantic)
Including Women in COVID-19 Decision-Making
Operation 50/50: Women’s perspectives save lives (Women in Global Health)
Pandemic Preparedness and Response
A meta-analysis of the association between gender and protective behaviors in response to respiratory epidemics and pandemics (PLoS One)
Playing the long game: How a gender lens can mitigate harm caused by pandemics (Center for Global Development)
Strategic preparedness and response plan for the novel Coronavirus (WHO)
Gender and the Coronavirus outbreak (Council on Foreign relations)
Paying attention to women’s needs and leadership will strengthen COVID-19 response (UN Women)
Development and Humanitarian Settings
Gender implications of Covid-19 outbreaks in development and humanitarian settings (CARE)
Economic insecurity/employment
The coronavirus fallout may be worse for women than men. Here’s why. (World Economic Forum)
How will COVID-19 affect women and girls in low- and middle-income countries? (Center for Global Development)
African countries respond quickly to spread of COVID-19 (NPR)
COVID-19 and implications for inclusive economic empowerment in CARICOM: Policy and programme considerations (UN Women Caribbean Multi-Country Office)
Pandemic: Informal workers urgently need income replacement — and more protections (WIEGO)
How the COVID-19 pandemic will affect informal workers: Insights from Kenya (The Conversation)
Domestic Violence
Reports from China indicate rise in domestic violence (Axios)
Home is not a safe place for everyone (Huffington Post)
Frequently Asked Questions - COVID-19 and family violence (The Lookout)
Health
Health-care workers
PES Women: Women are on the front line of the Corona-crisis, yet gender-issues are being ignored (PES)
COVID-19: Protecting health-care workers (The Lancet)
Needs of female medical workers overlooked in coronavirus fights, advocates say (Inkstone)
Sexual and Reproductive Health
The COVID-19 outbreak: Potential fallout for sexual and reproductive health and rights (Guttmacher Institute)
Pregnancy
What are the risks of COVID-19 infection in pregnant women? (The Lancet)
Novel Coronavirus “COVID-19”: Special considerations for pregnant women( Kaiser Family Foundation policy brief)
Mental Health
Briefing note on addressing mental health and psychosocial aspects of COVID-19 outbreak (IASC)
By 3 April 2020, world COVID-19 confirmed cases surpassed 1 million. But without data that is disaggregated by sex, these numbers tell us only part of the story. They are insufficient for understanding the unique impact of the crisis on women as compared to men. We need far more sex-disaggregated data to tell us how the situation is evolving, including on differing rates of infection, differential economic impacts, differential care burdens, and the incidence of domestic violence and sexual abuse.
Given this imperative, UN Women is leading global data collection efforts to close this information and knowledge gap. In partnership with the public sector and non-state actors, we are supporting data collection efforts to ensure that all people, particularly the most vulnerable, are accounted for. Further, through UN Women’s global gender data programme, Women Count, UN Women works with national statistical offices to strengthen their capacity to collect and use gender-responsive data.
1. Is UN Women collecting primary data on COVID-19 and its gendered implications? To what end?
Yes. Various UN Women regional and country offices have, in some form or another, initiated data collection activities to measure the impact of COVID-19 on the lives of women and girls. Specifically through UN Women’s global gender data programme, Women Count, at least four regions are leading rapid assessment surveys. The general aim of the survey is to provide information on how the livelihoods and circumstances of women and men are affected by COVID-19. The results of the survey will also inform UN Women’s own programming to respond to the crisis, and our advocacy to improve the well-being of women and girls, during and after the pandemic.
The Asia and the Pacific Regional Office is rolling out a rapid assessment survey in at least seven countries, starting with the Philippines and extending to Pakistan, Bangladesh, Myanmar, Nepal, Thailand and Indonesia. The survey is available in regional languages widely used in these countries.
Three other regions – East and Southern Africa, Europe and Central Asia, and Western and Central Africa – have been finalizing and/or working on their survey tools and are in talks with countries that are interested in conducting the survey. In addition, at least three countries – Senegal, United Republic of Tanzania and Viet Nam – are exploring the possibility of including a module on COVID-19 impacts in planned surveys of their national statistical offices.
2. In looking at the gendered implications of COVID-19, what are the thematic areas being covered by the rapid assessment surveys?
The survey responses will cover the following common themes: knowledge of COVID-19, economic empowerment, access to basic services and safety, and unpaid care and domestic work. Some regions/countries have added questions based on their needs and priorities. These additional themes include: violence and safety, social protection, coping mechanisms, household food production, and disability/functional difficulty.
3. How will the rapid assessment survey be conducted?
Given the nature of COVID-19 and related mobility restrictions, traditional ways of collecting information, such as face-to-face interviews with groups or individuals, are currently not possible. We are thus giving participating countries several data collection options, focusing on the use of online or telephone data sources.
These can be done either as a stand-alone survey or a module on COVID-19 integrated to another survey already being planned or executed.
4. What is the target population of the survey? Is it only women and girls?
The rapid assessment survey will target both women and men, although the scope varies by country. For example, a number of countries are targeting all phone users (e.g. The Philippines). This is, however, limited to women and men phone subscribers. Some countries will be rolled out by governments and will cover a broader population beyond phone subscribers (e.g. Ukraine, Moldova and Pakistan).
5. Will the results provide the full picture of the impact of COVID-19 in a country?
No. The results will be representative of the population of phone subscribers only. In as much as we would like to make the survey as nationally representative as possible, we are very much limited by the data collection modalities.
6. How will the data of survey respondents be protected?
Data privacy is very important to us and we at UN Women are guided by the Principles Governing International Statistical Activities, particularly its confidentiality principle. That is: individual data collected will be kept strictly confidential and used exclusively for statistical purposes.
7. Where can we find the results of UN Women’s rapid assessment surveys on the gendered impacts of COVID-19?
The survey results, once available, will be published on the Women Count Data Hub. Preliminary results for Asia and the Pacific are now available as of 29 April.
8. What other relevant data is UN Women collecting on COVID-19 and gender?
UN Women’s COVID-19 resource page contains a live global tracker of cases (see the tab: The emerging picture), as well as regularly updated data on infections by sex, as well as by sex and age, including infections among health-care workers by sex. Provided to UN Women by the WHO, the total number of cases reported by sex may not reflect the current total number of cases, as they are reported from the date when sex-disaggregated data were last available. These may also only reflect a subset of data where countries have reported sex-disaggregated data.
In addition, UN Women has compiled a list of 29 indicators to support country-level assessments and gender within COVID-19 response plans. The indicators are grouped into 10 policy priority areas. For each, an array of relevant data, statistical indicators and other types of data are provided. Visitors to the page have the option to download the data in either Excel or PDF format. This page will be updated frequently, as more data and research become available, particularly on the gendered impacts of the pandemic and the efforts to address them.
Photo credit: Hospital Clínic/Francisco Àvia