
The global crisis triggered by the coronavirus (COVID-19) is deepening fast, leaving researchers and policymakers scrambling to collect and analyse data to grasp its impact on affected countries and territories – 214 and counting, with over xx million confirmed cases.
COVID-19 is an urgent health crisis, but one which will have massive global social and economic impacts that will reverberate for years to come. Disaggregated data will be critical to capture the pandemic’s full impacts on diverse individuals, communities and economies and to inform policy responses.
Even as new data and evidence is being gathered, clues about the differential impact for women and men are already clear from existing gender research, as well as through lessons from previous crises. Together, these provide a guide to what evidence needs to be collected now. And they demonstrate that a one-size-fits-all response will not suffice.
Capturing the immediate health impacts
Initial data show that men are more likely to die from COVID-19 than women. But researchers warn that the data are incomplete, inconsistent across countries and should be treated with caution. As we learn more, it may be that some groups of women are particularly vulnerable. For example, women make up 70% of health-care workers globally and 80% of nurses in most regions, roles in which they have particularly close and prolonged contact with sick patients.
Distribution of physicians and nurses, by sex
Source: WHO 2019, data from National Health Workers Accounts for 91 countries for physician data and 61 countries for nursing data.
It is, then, perhaps not surprising that in Spain, there have been more than twice as many cases of COVID-19 among female health-care workers, compared to their male counterparts.
The case of health-care workers in Spain

Source: UN Women calculations based on data from Spain’s Ministry of Health, "Análisis Epidemiológico COVID-19". Latest data available at 12:00 on 6 April 2020.
The health impact may affect women in other ways too. Experience from the Ebola and HIV crises in developing countries shows that, when health systems fail, it is women who step in as unpaid home-based caregivers, often with devastating impacts on their own health.
With all eyes focused on the capacity of health systems to deal with COVID-19, it is important to track what happens to other vital services upon which women depend for their lives. During the Ebola crisis, rates of maternal mortality spiked in West Africa, due to lack of basic obstetric care.
When designing policy responses, barriers to women’s access to healthcare also need to be taken into account. For example, across a sample of 57 developing countries, discriminatory social norms mean that less than one quarter (23%) of women report being the sole decision-maker when it comes to their own health.
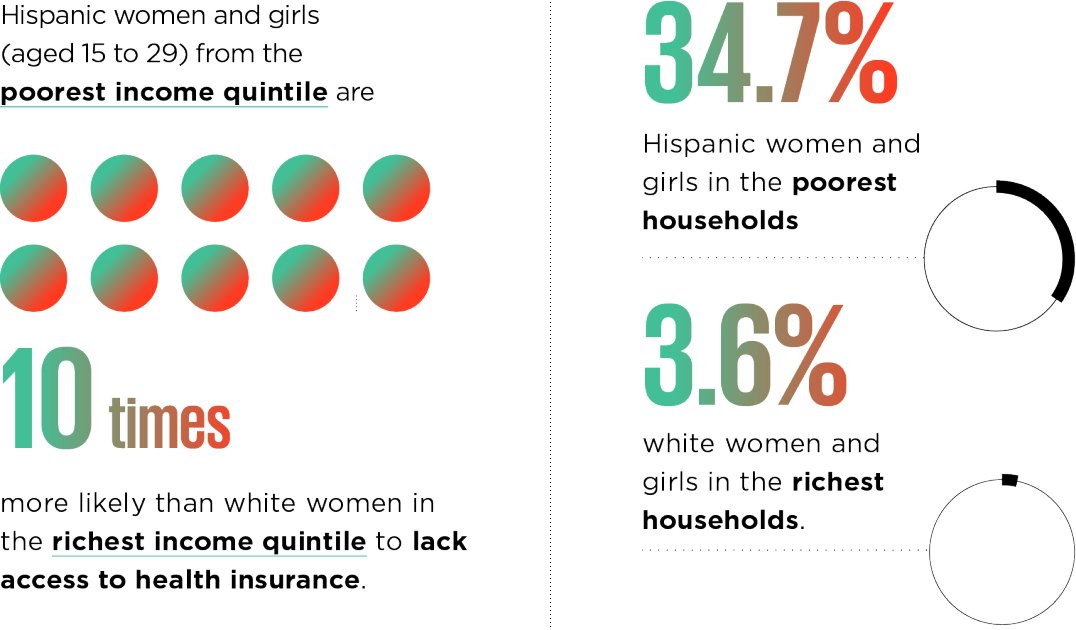
In countries where health care requires out-of-pocket payments or insurance, women from the poorest and most marginalized groups are likely to be deprived of vital care. In the USA, for example, in 2018 more than one third (34.7%) of Hispanic women in the poorest quintile lacked access to health insurance, compared to 3.6% of white women in the richest quintile.
Health insurance coverage and poverty in the US: The gap between Hispanic and white women
Source: UN Women analysis of American Community Survey
In common with previous crises, activists around the world report another grave threat to women’s health: the spiraling rates of intimate partner violence. With millions of people forced to stay in their homes, or self-isolating, many women are trapped with their abusers. Women’s organizations will be a key source of data and information on what’s needed to scale up vital services for survivors. Read more about this shadow pandemic.
Women caregivers at the forefront of the crisis
Beyond the health crisis, COVID-19 is quickly creating a care crisis. Health-care workers are justifiably in the spotlight right now, but the world’s women are also putting in billions of hours of care each day – both paid and unpaid – to enable the continuation of daily life.
Women are two thirds of the global paid care workforce, and the majority of paid caregivers for the elderly, in both facilities and home-based care. These low-paid workers need to be made visible to policymakers, to ensure their contribution is valued and they are protected, including with access to scarce personal protective equipment.
Feminization of the global care workforce
Source: Care work and care jobs for the future of decent work.
Women also do the bulk of unpaid care work in homes across the world, a workload that has intensified. This includes older women caring for frail partners and grandchildren. For those women able to work from home, the sudden need to home-school children has created a double (or triple) shift. Efforts are needed to capture the extent and intensity of women’s unpaid care work, so that it can be recognized and supported in the midst of the crisis, but also in the longer term.
Gendered economic repercussions
According to ILO estimates, the pandemic could cost between 5 million and 25 million jobs. Disaggregated data and targeted policies will be needed to ensure that the economic impacts are not shouldered disproportionately by women.
Globally, in 2019, 58.2% of women’s employment was in services, with rates of 80% or more in North America, in the European Union, Latin America and the Caribbean. This includes childcare, retail, hospitality and tourism, which are especially hard-hit by current restrictions. Widespread job losses will have long-term impacts for women’s economic independence and security.
A large share of women’s employment is in the informal economy, including in domestic work, jobs that lack labour rights and social protection, including health care, sick leave or unemployment benefits. In India, for example, upwards of 90% of women and men work in the informal economy in work such as street vending. In common with those in the gig economy in high-income countries, lockdowns to prevent the spread of disease mean these workers cannot earn a living.
Alternative sources of data, for example citizen generated data from informal and domestic workers’ organizations and networks can be leveraged to complement official data, to support policies and programmes to mitigate the economic fall-out of the COVID-19 crisis as it continues to unfold.
Gender data as a basis for the response
As countries face this crisis, efforts to address the pandemic should not jeopardize the fragile gains that have been made on gender equality. Continued progress on the 2030 Agenda for Sustainable Development depends on a policy response that builds more equal and resilient societies for the future. Researchers and policymakers need to learn from the past and prioritize collecting and reporting data, disaggregated by sex and other socio-economic characteristics, to ensure that marginalized women are not left even further behind.
The Women Count data hub is committed to compiling the best available gender analysis, and cutting-edge data sets, to support this vital global effort. Visit the COVID-19 resource page for updated gender data on the crisis.
Laura Turquet is the manager and co-author of UN Women’s flagship report, Progress of the World’s Women. For the past decade, she has worked at UN Women leading major research reports that inform the organization’s advocacy objectives and empower civil society and governments to seek and implement change. She is a co-founder of the UN Feminist Network and previously worked at various NGOs.
Sandrine A. Koissy-Kpein is a Statistics Specialist of UN Women, supporting the implementation of the global gender data programme, Women Count. She has been working in the United Nations system since 2017, with UNECA and UNDESA. Prior to that, she worked with academic research institutions and international NGOs. She has a background in development economics, econometrics and statistics.